
 It’s a great shame that my old schoolmate Mike Rachlis (we went to school together in Winnipeg) has to devote so much of his time and energy to countering the heavily financed misinformation campaigns that are trying to undermine Canada’s world class, universal, single-tier health care system, because he has some well-researched, innovative and proven ideas on how to make the Canadian system even better. For those unfamiliar with the Canadian situation, (mostly) US-based corporations are lobbying furiously to get our governments to abandon Canada’s public system and replace it with a US-style, two-tier, system, despite the fact that the US system provides most Americans (excluding the rich, overprivileged elite) with demonstrably poorer health care (Mike’s books have substantial data to back this assertion up), and are much less efficient and effective (health care costs consume 15% of US GDP compared to 9% in Canada, although millions of Americans are uninsured or underinsured, and the bureaucracy of the US system is stifling, with paperwork consuming as much as 40% of spending, far more than in Canada, to the point the NYT recently moaned that many Americans were so overwhelmed by the bureaucracy of the system that it was interfering with the quality of the care they receive). The reason for this lobbying is obvious and self-serving: Big Pharma and Big Medicine make substantially higher margins selling into the American system, and they want to con Canadians into believing that they should want such a system as well. So waiting times (although comparable to those in the US) are trotted out as evidence that Medicare is broken and the government is necessarily less capable of running a healthcare system than greedy private corporations. The con is working — the Conservative party in Canada and in Alberta, always willing to help generous foreign corporations line their own pockets in return for fat campaign contributions — is helping out with the misinformation campaign. So Mike has to focus much of his attention to countering the lies with hard facts, and his wise advice for improving the effectiveness of the Canadian system through innovations (most, ironically, borrowed from American community experiments) have received pathetically little public attention. The media dumb down the debate to “public vs. two-tier private” systems (Canadians consistently and overwhelmingly prefer the former, despite the money spent to try to convince them otherwise), and, except for the short-lived Romanow report (which most governments praised, but clearly don’t understand, as they have implemented few of the recommendations other than committing more money to the system), there has been almost no discussion of how to make the system even better. Mike’s newest book, Prescription for Excellence: How Innovation is Saving Canada’s Healthcare System (the choice of “is saving” rather than “could save” was presumably deliberate), is his latest attempt to bring attention to some of the practices that have been applied in various communities around the world, and which, if adopted by Canadian communities, could put an end to any doubts that Canada’s system is a world class model for other countries. Notice the focus is on communities. What Mike is calling for is sharing of information and best practices, and coordination of community-based healthcare initiatives, not massive centralized systems. He understands that networks work much better than hierarchies, but laments the lack of effective community-based networks in healthcare worldwide. The book lays out the principles and rules for effective healthcare established by the US National Institute of Medicine’s groundbreaking 2001 Crossing the Quality Chasm report: Principles: Health care should be:
Rules: Health care processes should be redesigned in accordance with the following ten rules:
Mike builds on these principles and rules to suggest specific improvements to Canada’s health-care system, at the community level, in each of these eight critical healthcare system stress points:
The recommendations are extensive, well-considered, practical, innovative, not difficult to implement, and illustrated with examples of where they have been successfully used. The biggest challenge, it seems to me, is the lack of autonomy of the community-based heathcare providers and systems, their ability, once they have had ‘aha’ moments and identified improvements they intuitively know will work, to actually implement them, free from top-down and bureaucratic interference. Nothing could be more discouraging than knowing what you need to do, and not being allowed to do it. That, and, for Americans, dealing with the infuriating and pervasive Moral Hazard Myth. |
Navigation
Collapsniks
Albert Bates (US)
Andrew Nikiforuk (CA)
Brutus (US)
Carolyn Baker (US)*
Catherine Ingram (US)
Chris Hedges (US)
Dahr Jamail (US)
Dean Spillane-Walker (US)*
Derrick Jensen (US)
Dougald & Paul (IE/SE)*
Erik Michaels (US)
Gail Tverberg (US)
Guy McPherson (US)
Honest Sorcerer
Janaia & Robin (US)*
Jem Bendell (UK)
Mari Werner
Michael Dowd (US)*
Nate Hagens (US)
Paul Heft (US)*
Post Carbon Inst. (US)
Resilience (US)
Richard Heinberg (US)
Robert Jensen (US)
Roy Scranton (US)
Sam Mitchell (US)
Tim Morgan (UK)
Tim Watkins (UK)
Umair Haque (UK)
William Rees (CA)
XrayMike (AU)
Radical Non-Duality
Tony Parsons
Jim Newman
Tim Cliss
Andreas Müller
Kenneth Madden
Emerson Lim
Nancy Neithercut
Rosemarijn Roes
Frank McCaughey
Clare Cherikoff
Ere Parek, Izzy Cloke, Zabi AmaniEssential Reading
Archive by Category
My Bio, Contact Info, Signature Posts
About the Author (2023)
My Circles
E-mail me
--- My Best 200 Posts, 2003-22 by category, from newest to oldest ---
Collapse Watch:
Hope — On the Balance of Probabilities
The Caste War for the Dregs
Recuperation, Accommodation, Resilience
How Do We Teach the Critical Skills
Collapse Not Apocalypse
Effective Activism
'Making Sense of the World' Reading List
Notes From the Rising Dark
What is Exponential Decay
Collapse: Slowly Then Suddenly
Slouching Towards Bethlehem
Making Sense of Who We Are
What Would Net-Zero Emissions Look Like?
Post Collapse with Michael Dowd (video)
Why Economic Collapse Will Precede Climate Collapse
Being Adaptable: A Reminder List
A Culture of Fear
What Will It Take?
A Future Without Us
Dean Walker Interview (video)
The Mushroom at the End of the World
What Would It Take To Live Sustainably?
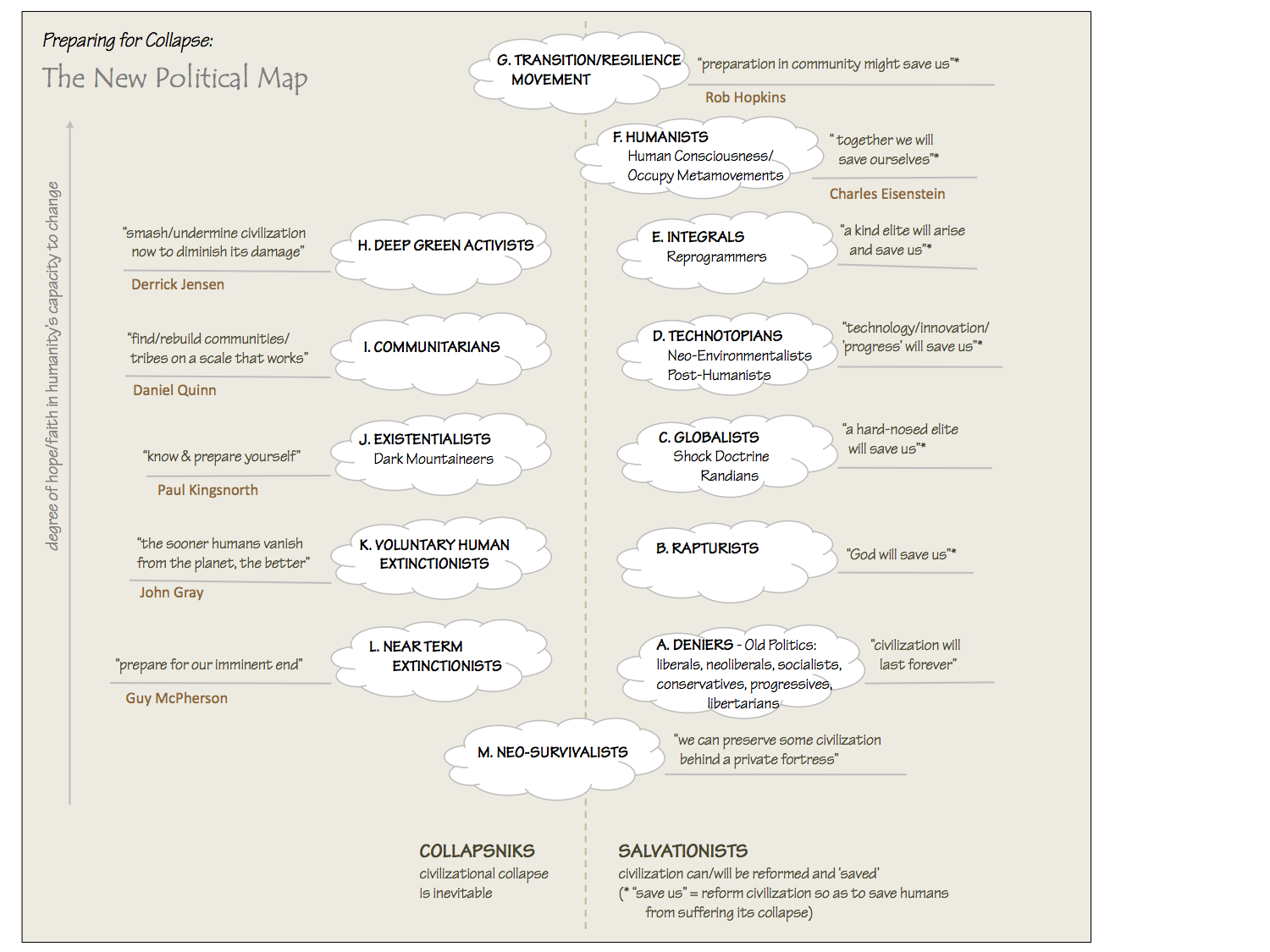
The New Political Map (Poster)
Beyond Belief
Complexity and Collapse
Requiem for a Species
Civilization Disease
What a Desolated Earth Looks Like
If We Had a Better Story...
Giving Up on Environmentalism
The Hard Part is Finding People Who Care
Going Vegan
The Dark & Gathering Sameness of the World
The End of Philosophy
A Short History of Progress
The Boiling Frog
Our Culture / Ourselves:
A CoVid-19 Recap
What It Means to be Human
A Culture Built on Wrong Models
Understanding Conservatives
Our Unique Capacity for Hatred
Not Meant to Govern Each Other
The Humanist Trap
Credulous
Amazing What People Get Used To
My Reluctant Misanthropy
The Dawn of Everything
Species Shame
Why Misinformation Doesn't Work
The Lab-Leak Hypothesis
The Right to Die
CoVid-19: Go for Zero
Pollard's Laws
On Caste
The Process of Self-Organization
The Tragic Spread of Misinformation
A Better Way to Work
The Needs of the Moment
Ask Yourself This
What to Believe Now?
Rogue Primate
Conversation & Silence
The Language of Our Eyes
True Story
May I Ask a Question?
Cultural Acedia: When We Can No Longer Care
Useless Advice
Several Short Sentences About Learning
Why I Don't Want to Hear Your Story
A Harvest of Myths
The Qualities of a Great Story
The Trouble With Stories
A Model of Identity & Community
Not Ready to Do What's Needed
A Culture of Dependence
So What's Next
Ten Things to Do When You're Feeling Hopeless
No Use to the World Broken
Living in Another World
Does Language Restrict What We Can Think?
The Value of Conversation Manifesto Nobody Knows Anything
If I Only Had 37 Days
The Only Life We Know
A Long Way Down
No Noble Savages
Figments of Reality
Too Far Ahead
Learning From Nature
The Rogue Animal
How the World Really Works:
Making Sense of Scents
An Age of Wonder
The Truth About Ukraine
Navigating Complexity
The Supply Chain Problem
The Promise of Dialogue
Too Dumb to Take Care of Ourselves
Extinction Capitalism
Homeless
Republicans Slide Into Fascism
All the Things I Was Wrong About
Several Short Sentences About Sharks
How Change Happens
What's the Best Possible Outcome?
The Perpetual Growth Machine
We Make Zero
How Long We've Been Around (graphic)
If You Wanted to Sabotage the Elections
Collective Intelligence & Complexity
Ten Things I Wish I'd Learned Earlier
The Problem With Systems
Against Hope (Video)
The Admission of Necessary Ignorance
Several Short Sentences About Jellyfish
Loren Eiseley, in Verse
A Synopsis of 'Finding the Sweet Spot'
Learning from Indigenous Cultures
The Gift Economy
The Job of the Media
The Wal-Mart Dilemma
The Illusion of the Separate Self, and Free Will:
No Free Will, No Freedom
The Other Side of 'No Me'
This Body Takes Me For a Walk
The Only One Who Really Knew Me
No Free Will — Fightin' Words
The Paradox of the Self
A Radical Non-Duality FAQ
What We Think We Know
Bark Bark Bark Bark Bark Bark Bark
Healing From Ourselves
The Entanglement Hypothesis
Nothing Needs to Happen
Nothing to Say About This
What I Wanted to Believe
A Continuous Reassemblage of Meaning
No Choice But to Misbehave
What's Apparently Happening
A Different Kind of Animal
Happy Now?
This Creature
Did Early Humans Have Selves?
Nothing On Offer Here
Even Simpler and More Hopeless Than That
Glimpses
How Our Bodies Sense the World
Fragments
What Happens in Vagus
We Have No Choice
Never Comfortable in the Skin of Self
Letting Go of the Story of Me
All There Is, Is This
A Theory of No Mind
Creative Works:
Mindful Wanderings (Reflections) (Archive)
A Prayer to No One
Frogs' Hollow (Short Story)
We Do What We Do (Poem)
Negative Assertions (Poem)
Reminder (Short Story)
A Canadian Sorry (Satire)
Under No Illusions (Short Story)
The Ever-Stranger (Poem)
The Fortune Teller (Short Story)
Non-Duality Dude (Play)
Your Self: An Owner's Manual (Satire)
All the Things I Thought I Knew (Short Story)
On the Shoulders of Giants (Short Story)
Improv (Poem)
Calling the Cage Freedom (Short Story)
Rune (Poem)
Only This (Poem)
The Other Extinction (Short Story)
Invisible (Poem)
Disruption (Short Story)
A Thought-Less Experiment (Poem)
Speaking Grosbeak (Short Story)
The Only Way There (Short Story)
The Wild Man (Short Story)
Flywheel (Short Story)
The Opposite of Presence (Satire)
How to Make Love Last (Poem)
The Horses' Bodies (Poem)
Enough (Lament)
Distracted (Short Story)
Worse, Still (Poem)
Conjurer (Satire)
A Conversation (Short Story)
Farewell to Albion (Poem)
My Other Sites

{kind=link}
{kind=link}
I read carefully through all of your items and point details and find that most of it is exemplary; however, the “evidence-based” decision making runs it off the rails. The evidence base is simply the newest jargonic method of enforcing conformity and compliance to the established system. Chuck out that “evidence-based” medicine crap and you’ve got a marvelous system of medicine there. Unfortunately, only the dunning process of “evidence-based” medicine is identifiable in our current system of medicne. The rest is completely alien to current practice. Too bad.
Good article, well reasoned, and outlines a nice core for a revamped health care system. As always, the devil is in the details.