
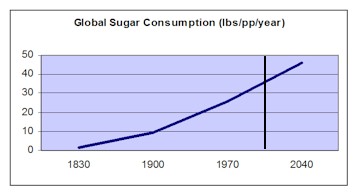
 Chart data from Irish sugar institute. EU/UK consumption per capita is about twice the global average above. North American consumption per capita has been consistently about four times the global average, of which more than half now comes from corn sweeteners. On top of that, a significant and rapidly growing proportion of the North American diet from sweeteners (as much as 20%) comes from artificial sweeteners. Our bodies die when one of five things happens:
There are few of us who aspire to find a ‘solution’ for the first cause. Eighty or a hundred years is a long time for any physical device with a lot of moving parts to endure, and the cost of replacing most of our bodies would be astronomical, and the process and results grotesque. Since the conquest of some of the biological agents like smallpox, tuberculosis, malaria and polio that have killed millions and even billions of humans, medical science (and we its patients) have become somewhat obsessed with causes 4 and 5, to the point we have come to believe that if we found ‘cures’ for these agents and defects we would all live long and healthy lives — as if causes 2 and 3 do not exist. Cause 2, self-inflicted trauma is not just suicide. When we abuse our bodies through the use of drugs, ingested, inhaled or injected, we are poisoning our bodies. Smoking could easily be seen as a form of slow suicide. When we deliberately choose to eat too much, too little, or an unhealthy mix of foods and beverages, we are knowingly poisoning ourselves, inflicting trauma on our bodies as surely as if we systematically cut our bodies with razor blades. Most of us are now addicted to the things we eat — fats, starches, sugars, salts, alcohol, caffeine and all the other unnatural substances that make us temporarily feel better but quickly get us craving more as the illusion of well-being wears off. It’s tempting to blame greedy corporations for our addictive diets, but the truth is we have craved these substances and the highs they give us since we first discovered them, and if these cravings were not satisfied by corporations we would find other ways to get them. Humans have created a ‘market’ economy and production system that can and does find a way to produce anything that people want — in fact that’s one of the reasons we invented that economy and system. The fact that this economy and system makes it easier for us to get addicted to more consumables that are toxic to our health simply explains why more humans die today of complications of obesity than of malnutrition. Cause 3, trauma induced by other humans is likewise not just homicide. We have so altered the chemistry of our air and water that it is changing the climate of the entire planet. It would be folly to think that such adulteration is not also massively affecting our bodies. The air we breathe, the water we drink and the foods we eat are laced with chemicals, both organic and inorganic, natural and man-made, that our bodies were never meant to ingest. Most of those chemicals have never been tested for toxological effect — there are simply too many for the testing agents to handle. Soaring rates of asthma, cancers and autism almost certainly have Cause 3 sources. They are the result of massive, collective human activity designed to make our lives better and, ironically, to make us healthier. While Cause 2 and Cause 3 are different, in many cases there is no easy way to differentiate between them. This is why we are willing to at least listen to people who blame Big Tobacco for addicting them to the product that is killing them, and who blame Big Agribusiness for addicting them to sugar and starch and subjecting their children to so many hormones and antibiotics in meat that there are no antibiotics left to treat them when they really get sick. I mentioned in an earlier article that some epidemiologists now believe AIDS and other diseases of those with compromised immune systems are not caused by HIV (a biological agent) but rather by inadvertent self-inflicted trauma — drugs favoured by homosexual males and toxins easily transmitted through shared and non-antiseptic needles. No one wants to hear this, because it would deprive the medical profession and Big Pharma of a great epidemic to solve, would make many of the sufferers of this terrible disease open to scapegoating, and would force science to admit a colossal blunder in diagnosis. And because it’s almost impossible to draw a line of responsibility between Cause 2 and Cause 3 traumas, it also raises the possibility and even probability that the poisons in our air, water and food are responsible for the damage to our immune systems that allow AIDS and the other immune-deficiency related epidemics ravaging much of the world. If poisoning by mining, air exhaust, food additives, antibiotics, dumping of wastes, and inability to clean up our water supplies are found to be the cause of auto-immune diseases and many cancers, a lot of people in high places could be looking at jail time for involuntary manslaughter. Not to mention a reputation in the history books as bigger mass-murderers than all the despots of human history combined. A reader writes: I have Chronic Fatigue Immune Dysfunction Syndrome (CFS/CFIDS) and HIV-Negative AIDS, idiopathic CD8 lymphocytopenia. With these two clinical diagnoses, I believe that makes me living proof that the AIDS-like CFS is transmissible, something that the medical establishment seems unable to admit or to acknowledge. I also believe it makes me living proof that Chronic Fatigue Syndrome and HIV-Negative AIDS are basically the same mysterious immune disorder.
Two years ago, after a heterosexual sexual encounter, I became seriously ill with what looks like the natural disease progression of AIDS. After an “acute infection” and a “period of asymptomatic health”, I have fallen extremely ill to an unrelenting, progressively-worsening AIDS-like demise. I can pinpoint exactly when I was infected with my “chronic viral syndrome of unknown etiology” and because the “acute infection” stage was so distinguishable, I can also pinpoint exactly when my undiagnosed illness left my body and infected yet another host. I am a link in a chain of systemically undiagnosed, sexually-connected, heterosexual sick people. Whatever I am currently dealing with, it strongly resembles classic textbook HIV/AIDS disease. But, to add to my inquiry, I also clinically satisfy the CDC’s criteria for the diagnosis of Chronic Fatigue Syndrome. As my blood indicates, my body is reacting to its undiagnosed foreign invader with: altered CD4/CD8 ratios; a rapid decline in lymphocyte percentages; a decline in CD3s; inflated LDH, CH50, Cortisol and segmented neutrophils levels; and a low T3 uptake. In accordance, my body is reacting to its immunodeficiency with severe and extensive abnormalities ranging from extreme weight loss and severe debilitating chronic fatigue to far more disturbing lung/thyroid tumors and AIDS-like opportunistic infections. Upon review of my medical file, you would see that I am an HIV-Negative AIDS (idiopathic CD8 lymphocytopenia) patient with a bleak future. Increasingly, I have become concerned that my systemic diagnosis is caught up in the treacherous politics of CFS and AIDS. Most people with CFS do not like to talk about the many symptoms and immune abnormalities that they share with AIDS patients. I also suspect that most ailing patients would rather be told that they have the very mysterious Chronic Fatigue Syndrome than to be told that they have AIDS. I have a Master’s degree. I am a director at my firm. I used to be a triathlete. I have never used IV drugs. I have never traveled abroad. I can count my sexual partners on two hands. Statistically speaking, I know that my undiagnosed infectious and communicable disease is not rare: so, you tell me, if they are not in the miscellaneous CFS category, where are all these other immunosuppressed people? Anyone with Chronic Fatigue Syndrome, who does not consider the possibility that CFS will eventually progress to a Non-HIV AIDS diagnosis, is very well trumping their own ability to diagnosis the root cause of their illness. Why isn’t CFS a reportable disease overseen by our public health department? Has anyone ever asked a CFS patient to epidemiologically track down all of their ex-sexual partners to see if any of them also suffer from an undiagnosed immune disorder? Why are we not reading about Non-HIV AIDS cases (and/or the AIDS-like nature of Chronic Fatigue Syndrome) on the front pages of every newspaper in America? And if CFS is Non-HIV AIDS, then, depending on who you believe, there are anywhere between 500,000 – 14,000,000 Americans out there with a transmissible illness. If that is what it truly is, our new form of AIDS dwarfs the ’Äòoriginal’Äô AIDS epidemic tenfold. I want honest answers for myself, for everyone who is suffering from this hideous illness, and especially for those who remain uninfected by my undiagnosed infectious and communicable disease. As worrisome as my health is to me, I am extremely troubled by the strong likelihood that more people are being infected every minute that HIV-Negative AIDS cases (like mine) are allowed to go undetected — especially if it turns out that AIDS and CFIDS are basically the same disorder. You can label my AIDS-like illness whatever you wish. I would even allow you to call it infectious-Chronic Fatigue Syndrome, even though it is utterly beyond my realm of comprehension as to how the medical establishment can generically name an entire disease paradigm based on just one (of my numerous) symptom(s). Regardless of how politics may try to dissuade or delude you, all you need to know is that my idiopathic immune dysfunction is infectious! It is contagious! And it is spreading, unleashed, in the world’s population! I am not afraid to say that I have AIDS without HIV — idiopathic CD8 lymphocytopenia — my second official clinical diagnosis. I am equally as unafraid of saying the most obvious thing about Chronic Fatigue Syndrome: It sure does look like AIDS to me. We talk openly about preparing for an impending Avian Flu pandemic. Why not talk about the HIV-Negative AIDS epidemic that already exists (and is spreading) amongst us? The writer believes that her disease itself is infectious, and she may well be right, but what if it is endemic in a society that ingests, voluntarily and involuntarily, millions of chemicals we have absolutely no idea of the long-range effects of on our bodies, and the infection agent is merely a catalyst that triggers the ‘syndrome’? Or what if it isn’t infectious at all, and it’s latent in all of us, just awaiting some other immune-system-challenging disease or some exhausting or stressful event in order to start wreaking havoc on our bodies? Are our bodies all fighting a constant life-and-death struggle with all the foreign, accumulating, interacting poisons that we ingest every time we breathe, drink or eat? Because Cause 2 and Cause 3 are so inseparable, it is tempting for politicians, health agencies and especially corporations, who might be liable once a causal link to their activities is established, to insist that there must be a Cause 4 for all these epidemic and fatal problems that would get them off the hook, and to fiercely resist even looking at other possible causes. There is plenty of circumstantial evidence that manufacturing, energy and resource industries (including many operations run by governments) are guilty of causing an untold number of deaths from Cause 3 negligence, and, while it would be a very tough case to prosecute, finding a Cause 4 for these deaths would both shift suspicion and refocus attention on the much easier cures for Cause 4 illnesses. So where does that leave us, the patients? The obvious lesson is not to depend on, or even particularly trust, those who have a vested interest in the outcome. We cannot and should not rely on governments, the NIH and its counterparts around the world, health care providers, Big Pharma, or of course polluting corporations to look after our interests — they are too busy looking after their own, which in some cases directly conflicts with ours. Here’s what we can do:
This doesn’t mean giving governments, health agencies, health practitioners or polluters an easy way out. In addition to the above, we should be lobbying governments and the health-care industry for more patient-centered approaches to health care: More focus on prevention (including tighter controls on pollution and on food additives and chemicals), on enabling greater self-care (in part by requiring the profession and Big Pharma to share more information with the public, and not just when it is favourable to their point of view and bottom line), and on more holistic analysis of health care problems (not just looking for Cause 4 and Cause 5 answers). We need to get rid of the conflicts of interest between governments, Big Pharma and patients — and resolve them in our favour. And we need to recapture the rights we lost a century ago to treat ourselves — as long as we are prepared to sign a waiver accepting full responsibility for the results, we should be able to self-administer drugs without a prescription and without regulatory approval. It’s ludicrous that the food junkies can push our kids to consume huge amounts of Aspartame and other poisons, but we can’t buy Codeine to help ease a friend’s enormous suffering unless we get written permission from a doctor. We’re old enough to take care of ourselves, and there’s plenty of evidence that if we don’t, we shouldn’t expect anyone else to. |
Navigation
Collapsniks
Albert Bates (US)
Andrew Nikiforuk (CA)
Brutus (US)
Carolyn Baker (US)*
Catherine Ingram (US)
Chris Hedges (US)
Dahr Jamail (US)
Dean Spillane-Walker (US)*
Derrick Jensen (US)
Dougald & Paul (IE/SE)*
Erik Michaels (US)
Gail Tverberg (US)
Guy McPherson (US)
Honest Sorcerer
Janaia & Robin (US)*
Jem Bendell (UK)
Mari Werner
Michael Dowd (US)*
Nate Hagens (US)
Paul Heft (US)*
Post Carbon Inst. (US)
Resilience (US)
Richard Heinberg (US)
Robert Jensen (US)
Roy Scranton (US)
Sam Mitchell (US)
Tim Morgan (UK)
Tim Watkins (UK)
Umair Haque (UK)
William Rees (CA)
XrayMike (AU)
Radical Non-Duality
Tony Parsons
Jim Newman
Tim Cliss
Andreas Müller
Kenneth Madden
Emerson Lim
Nancy Neithercut
Rosemarijn Roes
Frank McCaughey
Clare Cherikoff
Ere Parek, Izzy Cloke, Zabi AmaniEssential Reading
Archive by Category
My Bio, Contact Info, Signature Posts
About the Author (2023)
My Circles
E-mail me
--- My Best 200 Posts, 2003-22 by category, from newest to oldest ---
Collapse Watch:
Hope — On the Balance of Probabilities
The Caste War for the Dregs
Recuperation, Accommodation, Resilience
How Do We Teach the Critical Skills
Collapse Not Apocalypse
Effective Activism
'Making Sense of the World' Reading List
Notes From the Rising Dark
What is Exponential Decay
Collapse: Slowly Then Suddenly
Slouching Towards Bethlehem
Making Sense of Who We Are
What Would Net-Zero Emissions Look Like?
Post Collapse with Michael Dowd (video)
Why Economic Collapse Will Precede Climate Collapse
Being Adaptable: A Reminder List
A Culture of Fear
What Will It Take?
A Future Without Us
Dean Walker Interview (video)
The Mushroom at the End of the World
What Would It Take To Live Sustainably?
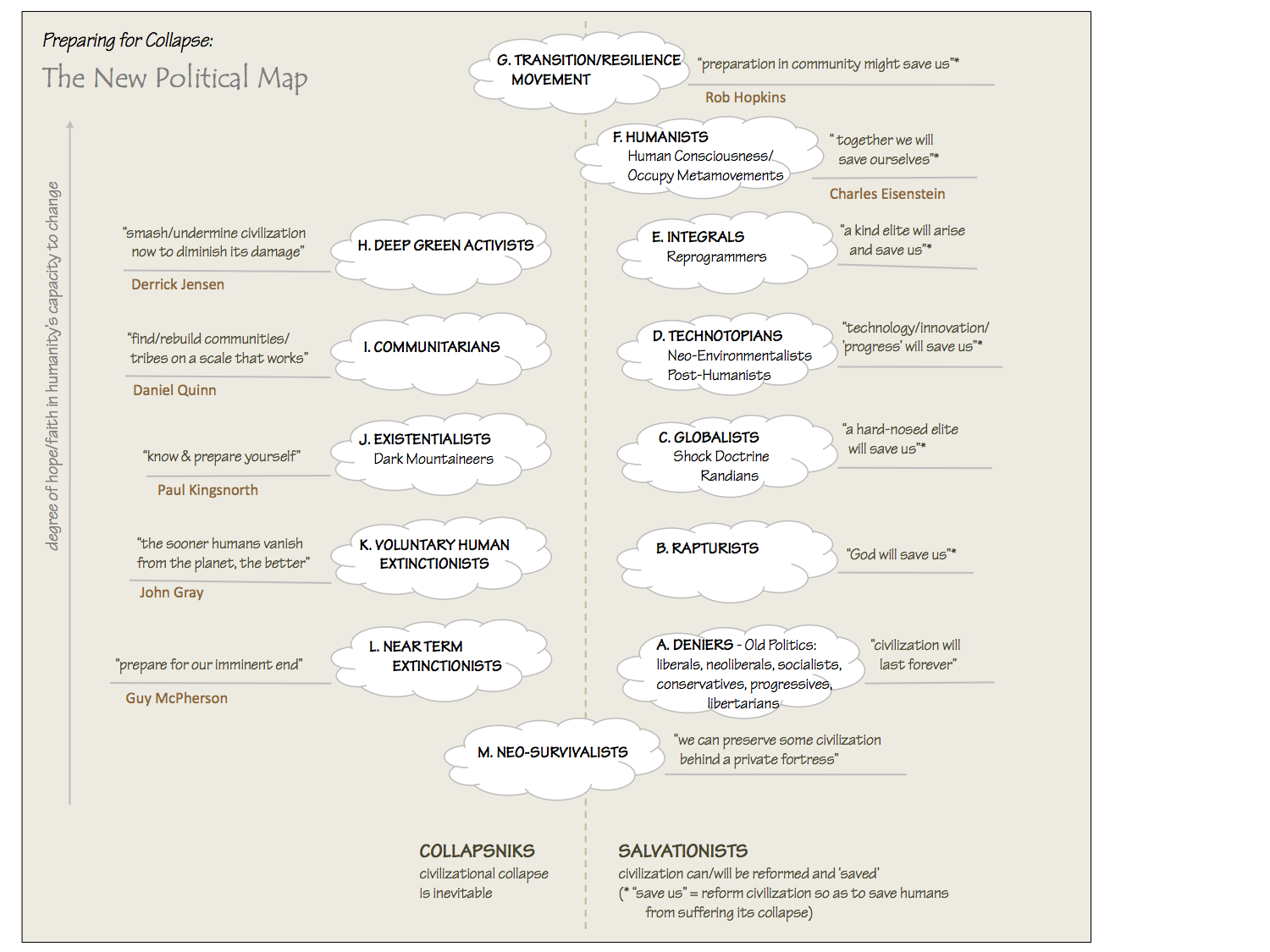
The New Political Map (Poster)
Beyond Belief
Complexity and Collapse
Requiem for a Species
Civilization Disease
What a Desolated Earth Looks Like
If We Had a Better Story...
Giving Up on Environmentalism
The Hard Part is Finding People Who Care
Going Vegan
The Dark & Gathering Sameness of the World
The End of Philosophy
A Short History of Progress
The Boiling Frog
Our Culture / Ourselves:
A CoVid-19 Recap
What It Means to be Human
A Culture Built on Wrong Models
Understanding Conservatives
Our Unique Capacity for Hatred
Not Meant to Govern Each Other
The Humanist Trap
Credulous
Amazing What People Get Used To
My Reluctant Misanthropy
The Dawn of Everything
Species Shame
Why Misinformation Doesn't Work
The Lab-Leak Hypothesis
The Right to Die
CoVid-19: Go for Zero
Pollard's Laws
On Caste
The Process of Self-Organization
The Tragic Spread of Misinformation
A Better Way to Work
The Needs of the Moment
Ask Yourself This
What to Believe Now?
Rogue Primate
Conversation & Silence
The Language of Our Eyes
True Story
May I Ask a Question?
Cultural Acedia: When We Can No Longer Care
Useless Advice
Several Short Sentences About Learning
Why I Don't Want to Hear Your Story
A Harvest of Myths
The Qualities of a Great Story
The Trouble With Stories
A Model of Identity & Community
Not Ready to Do What's Needed
A Culture of Dependence
So What's Next
Ten Things to Do When You're Feeling Hopeless
No Use to the World Broken
Living in Another World
Does Language Restrict What We Can Think?
The Value of Conversation Manifesto Nobody Knows Anything
If I Only Had 37 Days
The Only Life We Know
A Long Way Down
No Noble Savages
Figments of Reality
Too Far Ahead
Learning From Nature
The Rogue Animal
How the World Really Works:
Making Sense of Scents
An Age of Wonder
The Truth About Ukraine
Navigating Complexity
The Supply Chain Problem
The Promise of Dialogue
Too Dumb to Take Care of Ourselves
Extinction Capitalism
Homeless
Republicans Slide Into Fascism
All the Things I Was Wrong About
Several Short Sentences About Sharks
How Change Happens
What's the Best Possible Outcome?
The Perpetual Growth Machine
We Make Zero
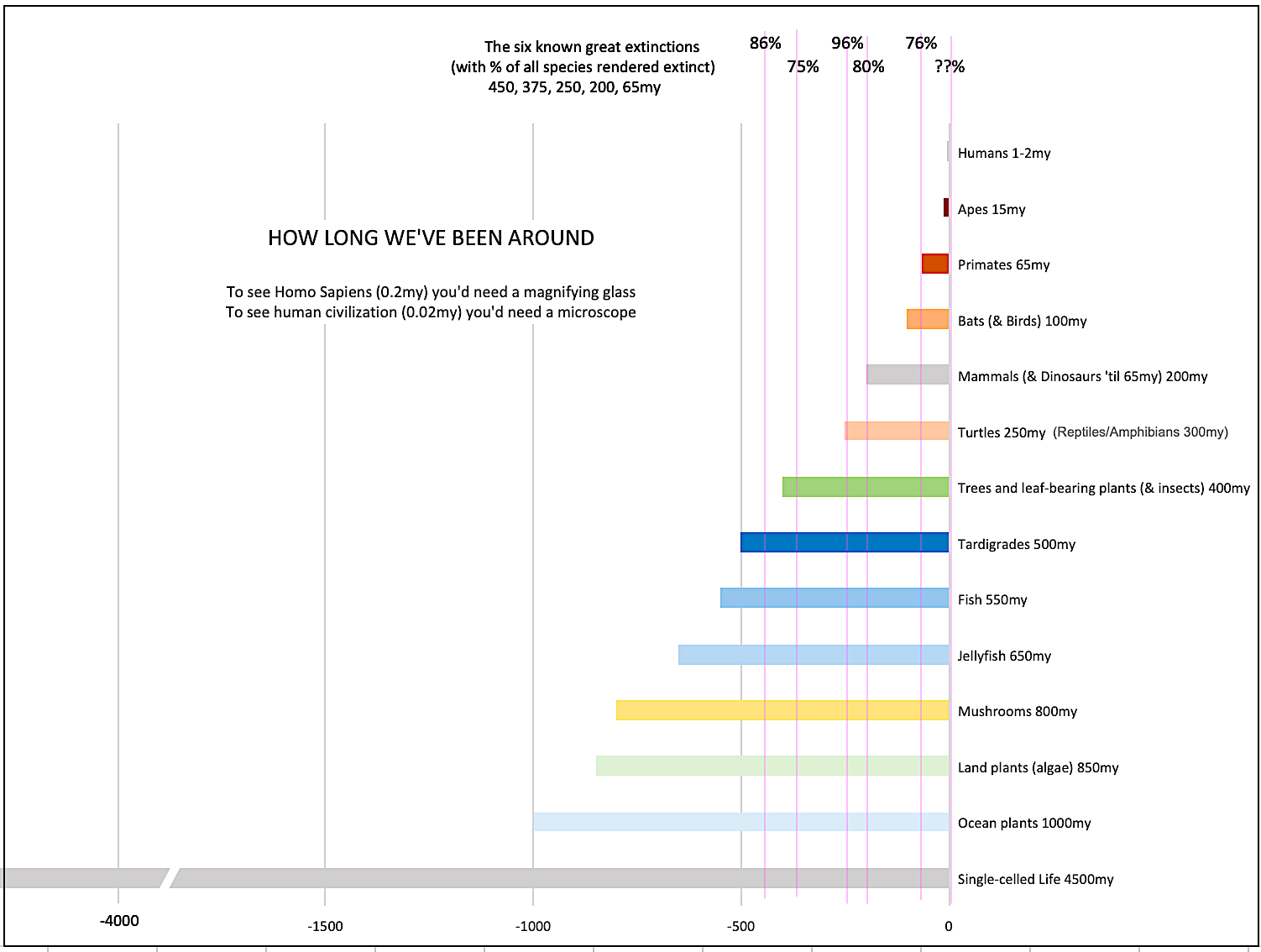
How Long We've Been Around (graphic)
If You Wanted to Sabotage the Elections
Collective Intelligence & Complexity
Ten Things I Wish I'd Learned Earlier
The Problem With Systems
Against Hope (Video)
The Admission of Necessary Ignorance
Several Short Sentences About Jellyfish
Loren Eiseley, in Verse
A Synopsis of 'Finding the Sweet Spot'
Learning from Indigenous Cultures
The Gift Economy
The Job of the Media
The Wal-Mart Dilemma
The Illusion of the Separate Self, and Free Will:
No Free Will, No Freedom
The Other Side of 'No Me'
This Body Takes Me For a Walk
The Only One Who Really Knew Me
No Free Will — Fightin' Words
The Paradox of the Self
A Radical Non-Duality FAQ
What We Think We Know
Bark Bark Bark Bark Bark Bark Bark
Healing From Ourselves
The Entanglement Hypothesis
Nothing Needs to Happen
Nothing to Say About This
What I Wanted to Believe
A Continuous Reassemblage of Meaning
No Choice But to Misbehave
What's Apparently Happening
A Different Kind of Animal
Happy Now?
This Creature
Did Early Humans Have Selves?
Nothing On Offer Here
Even Simpler and More Hopeless Than That
Glimpses
How Our Bodies Sense the World
Fragments
What Happens in Vagus
We Have No Choice
Never Comfortable in the Skin of Self
Letting Go of the Story of Me
All There Is, Is This
A Theory of No Mind
Creative Works:
Mindful Wanderings (Reflections) (Archive)
A Prayer to No One
Frogs' Hollow (Short Story)
We Do What We Do (Poem)
Negative Assertions (Poem)
Reminder (Short Story)
A Canadian Sorry (Satire)
Under No Illusions (Short Story)
The Ever-Stranger (Poem)
The Fortune Teller (Short Story)
Non-Duality Dude (Play)
Your Self: An Owner's Manual (Satire)
All the Things I Thought I Knew (Short Story)
On the Shoulders of Giants (Short Story)
Improv (Poem)
Calling the Cage Freedom (Short Story)
Rune (Poem)
Only This (Poem)
The Other Extinction (Short Story)
Invisible (Poem)
Disruption (Short Story)
A Thought-Less Experiment (Poem)
Speaking Grosbeak (Short Story)
The Only Way There (Short Story)
The Wild Man (Short Story)
Flywheel (Short Story)
The Opposite of Presence (Satire)
How to Make Love Last (Poem)
The Horses' Bodies (Poem)
Enough (Lament)
Distracted (Short Story)
Worse, Still (Poem)
Conjurer (Satire)
A Conversation (Short Story)
Farewell to Albion (Poem)
My Other Sites

{kind=link}
{kind=link}
Thank you for posting this wise and thoughtful commentary. As a late-onset Crohn’s disease patient, the subject of responsibility–personal and social–regarding immune system disease is of great importance to me. While there is a genetic component, late-onset Crohn’s in a patient with a parent (i.e., me) who experience early-onset is rare, and probably more attributable to environmental factors than genetic. I cop to having lived with astronomical levels of stress, for which I take full responsibility; in addition, my attempts at guarding and maintaining my general health prior to onset (which was, probably entirely due to genetics, excellent) was spotty, at best.Three and a half years later, I’m doing far better thanks to a “clean” diet (Specific Carbohydrate Diet, or SCD) that has worked wonders for Crohn’s and UC patients. What is also striking about it is the anecdotal evidence that it also aids patients with MS and children with autism. More than ever, I am convinced that our environment in general and what we pick and choose to ingest from it in particular are hugely responsible for the compromising of our immune systems and ill health. Weaker now than I was before, I see the effects of even the slightest “bad” food intake.I think items #1 – 4 are most critical for people starting out on the curve; item #5 is especially important for us cranks who still meet with the stone-faced disbelief of our representatives of the medical-industrial complex. Addressing things from the other side–i.e., getting more doctors to admit that they don’t know as much as they’d sometime like us to think–is a topic for another post entirely.
Oh–one more salient point I forgot to mention. The number one culprit in the fight to control Crohn’s & UC: di- and polysaccharides.
What about trying “Ayurveda”. It is not a magic cure, but maybe could render a better quality of life, and of course looking for certified organic food products. Changing the pH, the acid/alkalin range of our body chemistry, ( communicatrix, I guess that is what the you are doing with the mentioned diet) might help a lot.Macrobiotics is also a radical alternative – not as specific as Ayurveda.Better consult an Ayurvedic Doctor.—In countries like mine where regulations in the use of petsticides are not respected, poisoning through food is a terrible unknown drama. While nutricional programs say for instance “tomatos have a high range of antioxidants andx,x,x .. people beging to eat more and more tomatoes….. while tomatoes are being cured with the most toxic systemic pesticides….degenerative deseases, virus mutations…. a medicine that really knows not what to do (only produce expensive medicines that really cure nothing)an unemphatic, unhuman, agricultural and farming practices……¿what to do? Better look for developing local healthy production practices… which costs, unfortunatedly (at least for my country)are much more expensive for low income families… The air we breath, the water we drink, the food we eat…. everything that comes inside our organisms as well as to the organisms of the plants and animals we and Gaia feed of….. ¿what to do?
I’m having a hard time with these AIDS-not-HIV related posts, Dave. I’m not current, but once was, with this research — as I’ve lost more than one loved person to this disease. Do you have such confidence in your sources on this that you are willing to disbelieve virtually the entire medical community? If you were writing on evolution, would you be so credulous? And you know, I usually trust you absolutely.
SB, it appears to me you’re edging into the territory of credibility and influence. When I read these posts I find myself pondering not only the medical,scientific questions, but the mechanisms of credibility and influenceas well.How does credibility work?How does influence work?Who has been influenced, so far, by the articles SB noted? And why?Who still needs to be influenced if an AIDS anti-establishment is to achieve its apparent goal?If those are two different audiences, would it be worthwhile to consider two different mechanisms of credibility and influence?
Thanks for the comments, everyone. I’m not done with this subject yet, but I’m awaiting some additional information.
Thankyou for sharing this article.So many people suffer with undiagnosed illnesses/symptomsDoctors need more education on these matters