
As we head into another winter season of the pandemic, there are a number of scenarios that might play out from here. We are still enormously ignorant about many important facts about the virus and the pandemic, but some things are pretty clear:
- We are not going to eradicate the virus; it is just too transmissible and capable of rapid mutation. As such, everyone on the planet will either get the disease, be inoculated against it, or both. Masks, distancing, and shut-downs can effectively delay infection until each of us is inoculated, but unless you are inoculated it is just a matter of time before you contract the disease. Waiting will not reduce your risk.
- The death rate for the aged and for those with compromised immune systems is at least two orders of magnitude greater than that for healthy children, though no one is immune. This may change as additional variants emerge.
- The death rate in parts of Asia and Africa is at least one order of magnitude lower than that in affluent, sedentary nations with high rates of obesity and low exposure to other viruses in their childhood and in their everyday lives. Though, again, no part of the world is immune or sufficiently isolated to avoid endemic exposure and some risk of dying — this virus is that contagious.
- The vaccines have worked brilliantly, and have at least halved the number of deaths from the pandemic. Had they been introduced more quickly and universally, more than half of those who have died from the disease (and the vast majority of those who have died in the last six months) would likely have been spared.
- Global average vaccination rate is about 30%. In affluent nations the rate varies from about 40-80% by country, state, and age cohort, with an average of about 60%.
- There are no feasible ‘treatments’ for viral infections that might be used, now or in the future, to eliminate the need for vaccines. Viruses are staggeringly varied and quick to mutate, and antivirals are a hit-and-miss proposition with many dangerous side effects. And, as with antibiotics, the development of new antivirals raises the risk that viruses will emerge that are immune to them as well, eliminating their value even in the most desperate cases.
- Globally, the pandemic continues unabated, with about 10-20,000 people dying of it every day, and roughly three million new infections every day. This is about the average rate of deaths and new infections that the disease has produced since its very start eighteen months ago.
- After a year of remarkable stability, the last eight months have seen some dramatic mutations in the virus, all of them for the worse. A recent study described by NPR concluded that “SARS-CoV-2’s rate of adaptation is remarkably high right now, roughly four times higher for SARS-CoV-2 than it is even for seasonal flu, which changes so fast that people can be vulnerable to it each year.” NPR’s report goes on: “This fast evolution has immense implications, many scientists say. It essentially dashes the hopes of eradicating SARS-CoV-2 in the U.S. or even in smaller communities. As with the flu, the coronavirus will likely be able to reinfect people over and over again. It will keep returning year after year. ‘Eventually everyone will be exposed to SARS-CoV-2,’ says Dr. Abraar Karan, who’s an infectious disease specialist at Stanford University. ‘It’s just a matter of whether you’re exposed when you’re fully vaccinated or when you’re not vaccinated.’ “
- Between a third and an eighth of those infected with the disease have symptoms of chronic or permanent injury from damage caused by the disease, to the respiratory, neurological, cardiopulmonary and gastro-intestinal systems of the body, and/or to the brain and other organs. Even if most of these “long CoVid” symptoms eventually ease, the cost in terms of lost healthy life, lost work time, support health costs, and shortened overall life, will be astronomical.
- As the frequency and complexity of pandemic diseases continues to accelerate in the 21st century, we can expect more, and more severe, pandemics in the years ahead.
- The complexity of our global systems is such that we will not be able to eliminate or even significantly diminish the causes that underlie pandemics — massive-scale factory farming; the cultivation, harvesting and exposure to exotic animals that are reservoirs for most pandemic viruses; and the invasion and destruction of the world’s last wilderness areas that currently contain many more unknown pathogens.
- There is almost no evidence that we — the leaders and members of our political, social, economic, and health systems — have learned any lessons from CoVid-19 that will significantly change our response to the next pandemic. We are likely to repeat the same mistakes we are continuing to make now, and because the next pandemic is (statistically) likely to come from animal-to-human species-gap transmission from a factory farm reservoir, we may take even longer to respond to its more complex transmission mechanisms than we did this time around.
Some other things are completely unclear, and are likely to remain so, perhaps forever:
- As with the 1918 pandemic, we will probably never know how many people caught the disease, or how many died from it, and hence, we will never know even approximately what the Infection Fatality Rate (IFR) for the disease is. There are credible estimates that range from 8-17M deaths so far, 15-60% of the population infected so far, and hence an IFR anywhere in the 0.17-1.7% range.
- As with the 1918 pandemic, we have no idea how the disease will mutate from here on. A radical mutation of the 1918 virus created a late, devastating wave that killed four times as many as the earlier waves, and targeted especially the young and healthy, precipitating a violent immune system reaction that killed its victims — those with strong immune systems were essentially killed by their own reactions, not by any action of the virus itself. Such a mutation of the SARS-CoV-2 virus is entirely possible, especially as the disease’s spread continues largely unabated.
- We don’t know how severe the effects of “Long CoVid” will be, nor what they will be, nor how long they will last, among the likely billions who will bear the scars of this disease, some in ways they do not yet know and cannot even imagine.
- We don’t know how this pandemic originated. While there are some plausible theories of human incompetence causing it, there are far more tenable theories that the virus was transmitted by a bat directly to a human, and that such accidents, while rarely as devastating as CoVid-19 turned out to be, happen all the time.
- We don’t know how the virus affects us, makes us ill, and kills us. We are still fighting the symptoms, not the mechanism that gives rise to them, because the virus seems to have many, many, complex, inconsistent and unpredicted effects on many different parts of our bodies.
- We don’t know how long the vaccines, and getting infected, will continue to offer protection against new infections, and what effect “booster” shots will have on immunity to infection and reinfection.
- We don’t know what proportion of the hold-outs will get vaccinated, and when, either because of work mandates (there’s some evidence at more than 80% of holdouts begrudgingly get vaccinated when their job is on the line), or because, in many less affluent countries, vaccines are finally made available when they haven’t been to date. This could make a huge difference on the duration of the pandemic and the likelihood of new, virulent variants emerging.
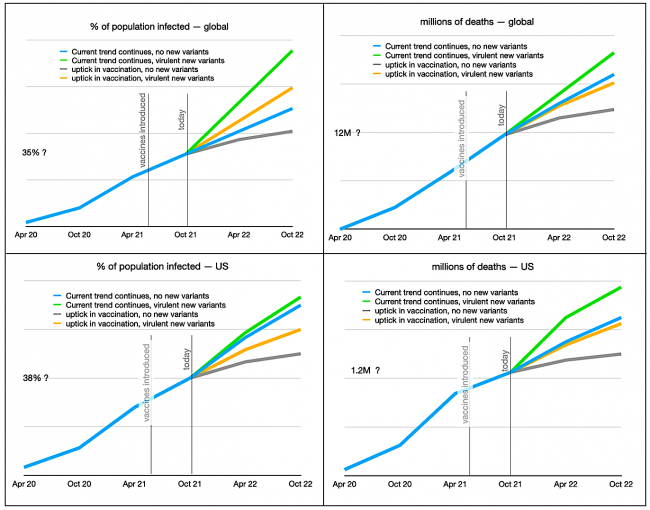
So that leaves us with the possible scenarios outlined in the charts above. What they suggest is that, far from the pandemic being close to its end, as we’d hoped when the vaccines were introduced, we’re really not far beyond the middle. Few countries have achieved the 80-90% vaccination rates needed to achieve herd immunity, especially with borders opening, mask mandates being dropped, and the extraordinary transmissibility of the Delta variant. The blue “business as usual” projections in these charts presume that vaccine take-up among the unvaccinated will remain sluggish, as we enter the winter season in the Northern Hemisphere which last year saw a sharp upward spike in CoVid-19 infections and deaths. It suggests that a year from now we will not be much further ahead than we are now in terms of getting the pandemic under control.
If there is a dramatic uptick in vaccine take-up, and if the aged and vulnerable get booster shots, then a year from now (grey lines) we might finally be able to do everything we could do before the pandemic, though we will probably still be using masks as prophylactics indoors with strangers or in areas of the country and world with continuing high case rates. That’s the best case scenario.
If there is a new, more virulent variant (and with current low vaccination rates there is lots of time and lots of places for one to emerge), then all bets are off. The radically virulent variant that emerged in 1918 after the initial waves put everything back to square one, as it primarily sickened and killed the young and the healthy, notably children, and this is the age cohort that would be most vulnerable to such a variant now, since their vaccination rate is very low almost everywhere in the world. We could see infection and death rates much higher than what we have seen to date.
Why is this going on so long? It’s a combination of factors. Our modern way of living and travelling allows new viruses to reach every part of the world with unprecedented speed. Our lifestyle in affluent nations prevents our immune systems from learning healthy and powerful responses to pathogens, because of our nutritionally poor, unvaried diets and our excessive use of antibiotics and chemicals. Fear of governments and other authorities has increased public opposition to mandates and vaccines, and hence led to much lower rates of compliance with health authorities’ recommendations. Public health departments have been systematically starved of needed resources for research and preparedness for decades. And bad luck has also played a part — the accident of the virus’ first appearance, its extraordinary transmissibility, and more recently the rapid pace of its mutation.
While flu pandemics have tended to be short-lived, other viral pandemics (such as polio and AIDS) have gone on for years, even decades. Just as 9/11 may have permanently changed our experience of air travel, it is possible that CoVid-19 will usher in permanent changes in our social and work behaviour. The real surprise is that, with all the preconditions in place, it has taken so long for a pandemic to have as great a global impact as CoVid-19 has. If you were dreaming about a celebratory mask-burning to mark the end of the pandemic, best put such thoughts out of your mind for the foreseeable future.

{kind=link}
{kind=link}
Historian John Berry, author of The Great Influenza, has commented on the importance of governments maintaining the trust of the public when managing a pandemic.
In British Columbia that trust has been one of the very first collateral casualties of the pandemic, and as long as the pandemic persists it is going to be very very difficult — perhaps impossible — for government to restore that trust.
https://www.rochester.edu/newscenter/historian-john-barry-compares-covid-19-to-1918-flu-pandemic-454732/
Your statement that antivirals are not available is just not true.
Lots of substances both repurposed drugs, supplements, lozenges and gargles show great promise but have been systematically ignored by the public health establishment and most western countries.
There are for example several RCTs of medium quality showing remarkable effectiveness for nasal spray‘s and gargles in preventing and treating Covid. But these have been done largely in other countries and you don’t hear them in the United States. Why are we not doing simple to set up double blind tests of gargling with betadine, Listerine or other promising antivirals. It’s hard to conclude anything other than because it would go against the interests of big Pharma.
Herb, believe what you want to believe. When we have preventatives with extraordinary efficacy (vaccines), not using them and instead seeking possible treatments, none of which has demonstrated high efficacy, and none of which prevent this extraordinarily transmissible virus from continuing to spread, is IMO the height of lunacy. Betadine and listerine are antibiotics, not antivirals, and ivermectin is an anti-parasitic, not an antiviral. Using any of them is useless, just bad science and bad medicine.
An ounce of prevention truly is worth a pound of cure. Just ask any of the perhaps hundreds of millions who will have to deal with the horrific cost and lifelong suffering that Long CoVid inflicts on many of those infected, including many who were asymptomatic. It’s perfectly understandable to be frightened and suspicious of big corporate oligopolies and oppressive governments, and of something being injected in your body, but in this case we all have to set those concerns aside and take one for the team.
Re Point 6 and your reply to Herb: yes, ivermectin is an anti-parasitic drug but it has shown great promise in treating covid. Check out what happened in Uttar Pradesh State in India when they used it compared to next-door states which didn’t. Check out the work of Dr Tess Lawrie (evidence-based medicine) in the UK. Checkout the FLCCC alliance in the US. Over 64 studies have shown its efficacy in treating covid.
Mr. Pollard:
You are trying to understand something that may not be understandable because of the enormous number of variables involved. As time and understanding move ahead, more variables are added and the wished-for target (understanding) remains elusive.
You appear to have staked out a position in your reply to Herb, above. But it is just a position and not a final answer. Such answers have a way of cutting off thought but do have the benefit of comforting the self. And everyone needs comforting at times. Perhaps especially now.
David,
Thank you for this post. I recognize the amount of time, research, and thoughtfulness you have offered your readers. Reading your post today and with an unvaccinated friend on day six in the hospital, it’s a reminder to continue to use the precautionary principle.
I will be sharing this post with my network of friends.
This is the best, most comprehensive
Explanation of the past, present, future of
Covid I have seen!! This virus is real, deadly,
And is here to stay! Get vaccinated or get Covid.
Those are the choices. Remember, “An ounce
of prevention is worth a pound of cure”!
Thank you David!!
Dr Stephen Jay Smith
This piece is essentially
a puff piece from big Pharma, to justify what they have done what they want to continue doing, giving use booster shots every six months. If doctors had been allowed to do what doctors do, figure out the problem and come up with a solution, which many doctors did, then lives would not have had to have been lost. The exact opposite is true in regard to vaccinations. The more people who are vaccinated, the worse chance we have of stopping it.