
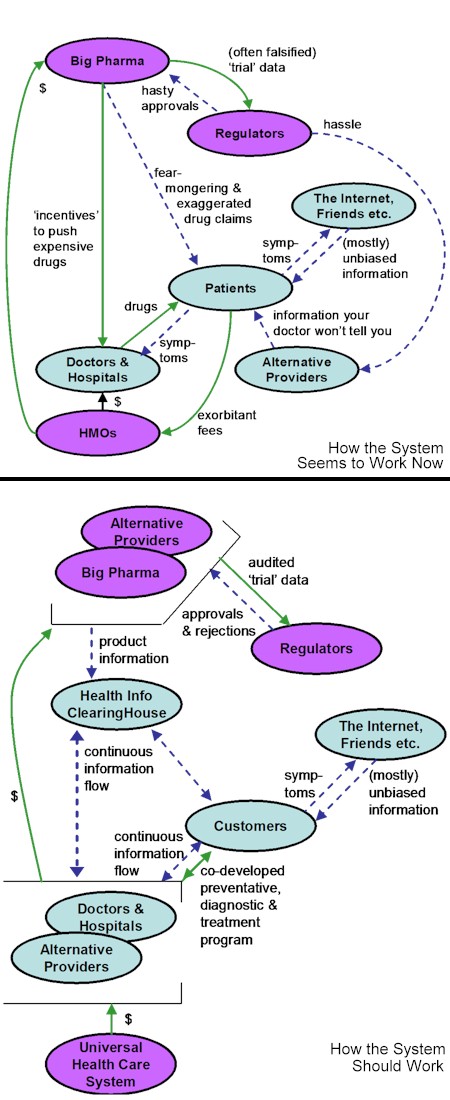
 Yesterday I commented on the intriguing health care ‘value chain’, shown above, that Verna Allee’s group has constructed, seen from the perspective of Big Pharma. This perspective assumes that ‘the patient’ is basically helpless, passive, ignorant and uninterested in taking an active role in the management of his/her own health. That’s a very patronizing perspective, though I admit I know many patients who give it credence. I would argue, however, that this is changing, and changing quickly. What is precipitating this change is:
Last week I contrasted, a bit simplistically, the traditional approach and the emerging ‘Edge’ approach to being healthy:
This emerging approach is entirely consistent with the recommendations of the US National Institute of Medicine’s 2001 Crossing the Quality Chasm report which laid out these ten ‘rules’ to govern effective health care:
So what would a health-care system ‘value network’ look like that honoured these rules? Certainly not like the one above. Here are two charts that show, first, how I think an increasing number of (cynical) patients see the ‘value network’ operating today, and then, below it, what a reformed health-care system ‘value network’ would/could/should look like:
The significant new ‘ingredient’ in the bottom chart, the Health Info ClearingHouse, is an example of what I have called a peer-to-peer information exchange. The ClearingHouse would be largely Internet-based (though also accessible through other media), not-for-profit, and not owned or controlled by anyone. It would aggregate and objectively assess health information provided by everyone in the system — customers (patients), doctors and other health-care providers, pharma companies, regulators and other government bodies etc. It would allow us to second-guess the hype we’re getting from for-profit providers and bureaucracies, get second opinions, and form support groups and share information and resources with other customers dealing with the same ailments. Under this system, as in most countries today other than the US, Big Pharma would no longer be able to ‘push’ its drugs through the mass media (“despite these 147 side-effects, ask your doctor if new overpriced toxic XanthamPlus is right for you!”) nor would it be able to bribe doctors with ‘incentives’ to prescribe its brands. The other big change would be in the relationship between doctors and other health-care providers and their customers (mere ‘patients’ no longer). The new relationship would be a continuous one, with factual information (data about customers’ health, analysis reports, new medical reports, etc.) being transmitted continuously between the customer and the health-care provider (perhaps even, as in some places in Japan now, automatically and electronically). The three-way information flows between customers, health-care providers and the ClearingHouse would enable the establishment of a co-developed ongoing personal program for every individual that would include (a) activities to prevent illnesses from occurring, (b) activities to self-diagnose illnesses in their very early stages, and (c) activities to treat illnesses when they occur. These would be joint activities with the customer actively engaged in the process. Such a system is almost a no-brainer: it would generally result in a healthier populace and much lower costs to the system. But its evolution has been, and will continue to be, blocked by the special interests who would lose out in such a system: Big Pharma would find less need and market for its products, and its influence in the system would be drastically reduced. The HMOs, of course, would be out of business. Many of the lawyers who make their living on both sides of patient-health-care-provider litigation would also be out of business, since along with greater control over their own health, customers would also have to accept more responsibility, and not be able to hide behind ignorance and helplessness when suing doctors and drug companies. Doctors with God-complexes would not handle such a system well. Predatory snake-oil and wonder-therapy ‘alternative’ health-care providers would find themselves exposed by the ClearingHouse. As you can see, then, there are plenty of reasons why the current dysfunctional system continues to squander our money and our health. And this is another complex system, that cannot be fixed by government fiat or by any group acting alone. We need to get to the system in the bottom chart above by evolutionary means. That evolution needs to start with bottom-up awareness, organization and information exchange, probably beginning with both (a) an insistence, when dealing with health-care providers, on complete two-way information exchange, total honesty and active customer involvement in all assessments and decisions, and (b) the establishment of the beginnings of what will eventually be the Health Information ClearingHouse. Instead of opting out of the system in favour of alternative medicine, we need to demand a greater role in our own health management from practitioners, and refuse to take no for an answer. My guess is that many practitioners will welcome rather than resist this change. In other words, we need to become our own holistic ‘general practitioner’. We cannot expect doctors to know what is happening, and what we are doing, in alternative health-care and in our own lives, unless we tell them. We need to tell everyone we involve in our health what everyone else we involve is doing and saying and prescribing, and what we are doing about it. That means that what our doctor, our physical and/or psychotherapist, our herbalist, our pharmacist, our personal trainer, our dietitian knows, they all should know, and we should know not only what they have told us to do, but why, and what else they considered and ruled out. And there, of course, is the rub. This requires more candour than a lot of us are willing to exhibit, and an investment in time and energy and learning that is more than many of us areprepared to make. But until we do, the system will remain dysfunctional and insolvent. And we’ll keep getting needlessly ill. |
Navigation
Collapsniks
Albert Bates (US)
Andrew Nikiforuk (CA)
Brutus (US)
Carolyn Baker (US)*
Catherine Ingram (US)
Chris Hedges (US)
Dahr Jamail (US)
Dean Spillane-Walker (US)*
Derrick Jensen (US)
Dougald & Paul (IE/SE)*
Erik Michaels (US)
Gail Tverberg (US)
Guy McPherson (US)
Honest Sorcerer
Janaia & Robin (US)*
Jem Bendell (UK)
Mari Werner
Michael Dowd (US)*
Nate Hagens (US)
Paul Heft (US)*
Post Carbon Inst. (US)
Resilience (US)
Richard Heinberg (US)
Robert Jensen (US)
Roy Scranton (US)
Sam Mitchell (US)
Tim Morgan (UK)
Tim Watkins (UK)
Umair Haque (UK)
William Rees (CA)
XrayMike (AU)
Radical Non-Duality
Tony Parsons
Jim Newman
Tim Cliss
Andreas Müller
Kenneth Madden
Emerson Lim
Nancy Neithercut
Rosemarijn Roes
Frank McCaughey
Clare Cherikoff
Ere Parek, Izzy Cloke, Zabi AmaniEssential Reading
Archive by Category
My Bio, Contact Info, Signature Posts
About the Author (2023)
My Circles
E-mail me
--- My Best 200 Posts, 2003-22 by category, from newest to oldest ---
Collapse Watch:
Hope — On the Balance of Probabilities
The Caste War for the Dregs
Recuperation, Accommodation, Resilience
How Do We Teach the Critical Skills
Collapse Not Apocalypse
Effective Activism
'Making Sense of the World' Reading List
Notes From the Rising Dark
What is Exponential Decay
Collapse: Slowly Then Suddenly
Slouching Towards Bethlehem
Making Sense of Who We Are
What Would Net-Zero Emissions Look Like?
Post Collapse with Michael Dowd (video)
Why Economic Collapse Will Precede Climate Collapse
Being Adaptable: A Reminder List
A Culture of Fear
What Will It Take?
A Future Without Us
Dean Walker Interview (video)
The Mushroom at the End of the World
What Would It Take To Live Sustainably?
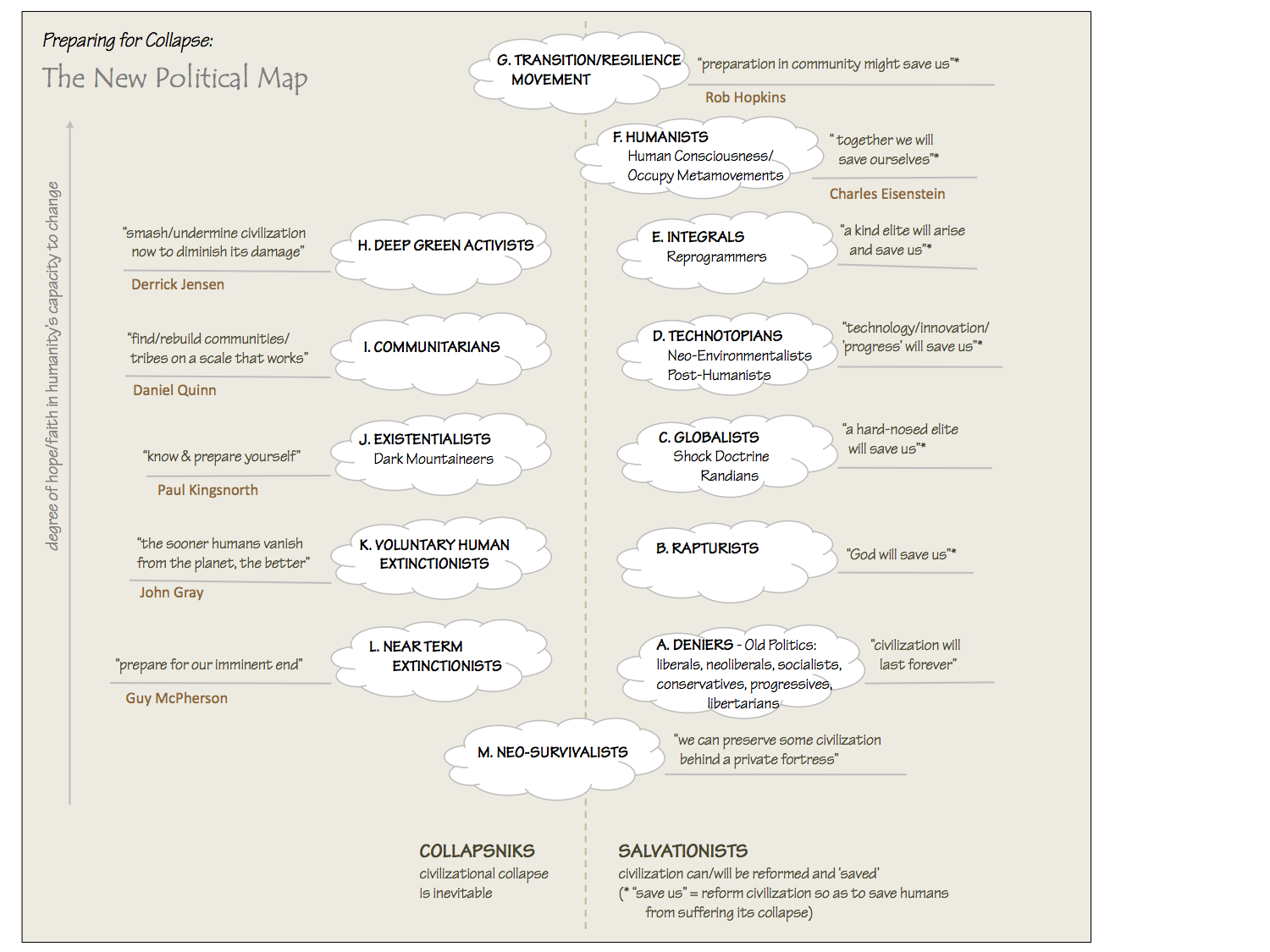
The New Political Map (Poster)
Beyond Belief
Complexity and Collapse
Requiem for a Species
Civilization Disease
What a Desolated Earth Looks Like
If We Had a Better Story...
Giving Up on Environmentalism
The Hard Part is Finding People Who Care
Going Vegan
The Dark & Gathering Sameness of the World
The End of Philosophy
A Short History of Progress
The Boiling Frog
Our Culture / Ourselves:
A CoVid-19 Recap
What It Means to be Human
A Culture Built on Wrong Models
Understanding Conservatives
Our Unique Capacity for Hatred
Not Meant to Govern Each Other
The Humanist Trap
Credulous
Amazing What People Get Used To
My Reluctant Misanthropy
The Dawn of Everything
Species Shame
Why Misinformation Doesn't Work
The Lab-Leak Hypothesis
The Right to Die
CoVid-19: Go for Zero
Pollard's Laws
On Caste
The Process of Self-Organization
The Tragic Spread of Misinformation
A Better Way to Work
The Needs of the Moment
Ask Yourself This
What to Believe Now?
Rogue Primate
Conversation & Silence
The Language of Our Eyes
True Story
May I Ask a Question?
Cultural Acedia: When We Can No Longer Care
Useless Advice
Several Short Sentences About Learning
Why I Don't Want to Hear Your Story
A Harvest of Myths
The Qualities of a Great Story
The Trouble With Stories
A Model of Identity & Community
Not Ready to Do What's Needed
A Culture of Dependence
So What's Next
Ten Things to Do When You're Feeling Hopeless
No Use to the World Broken
Living in Another World
Does Language Restrict What We Can Think?
The Value of Conversation Manifesto Nobody Knows Anything
If I Only Had 37 Days
The Only Life We Know
A Long Way Down
No Noble Savages
Figments of Reality
Too Far Ahead
Learning From Nature
The Rogue Animal
How the World Really Works:
Making Sense of Scents
An Age of Wonder
The Truth About Ukraine
Navigating Complexity
The Supply Chain Problem
The Promise of Dialogue
Too Dumb to Take Care of Ourselves
Extinction Capitalism
Homeless
Republicans Slide Into Fascism
All the Things I Was Wrong About
Several Short Sentences About Sharks
How Change Happens
What's the Best Possible Outcome?
The Perpetual Growth Machine
We Make Zero
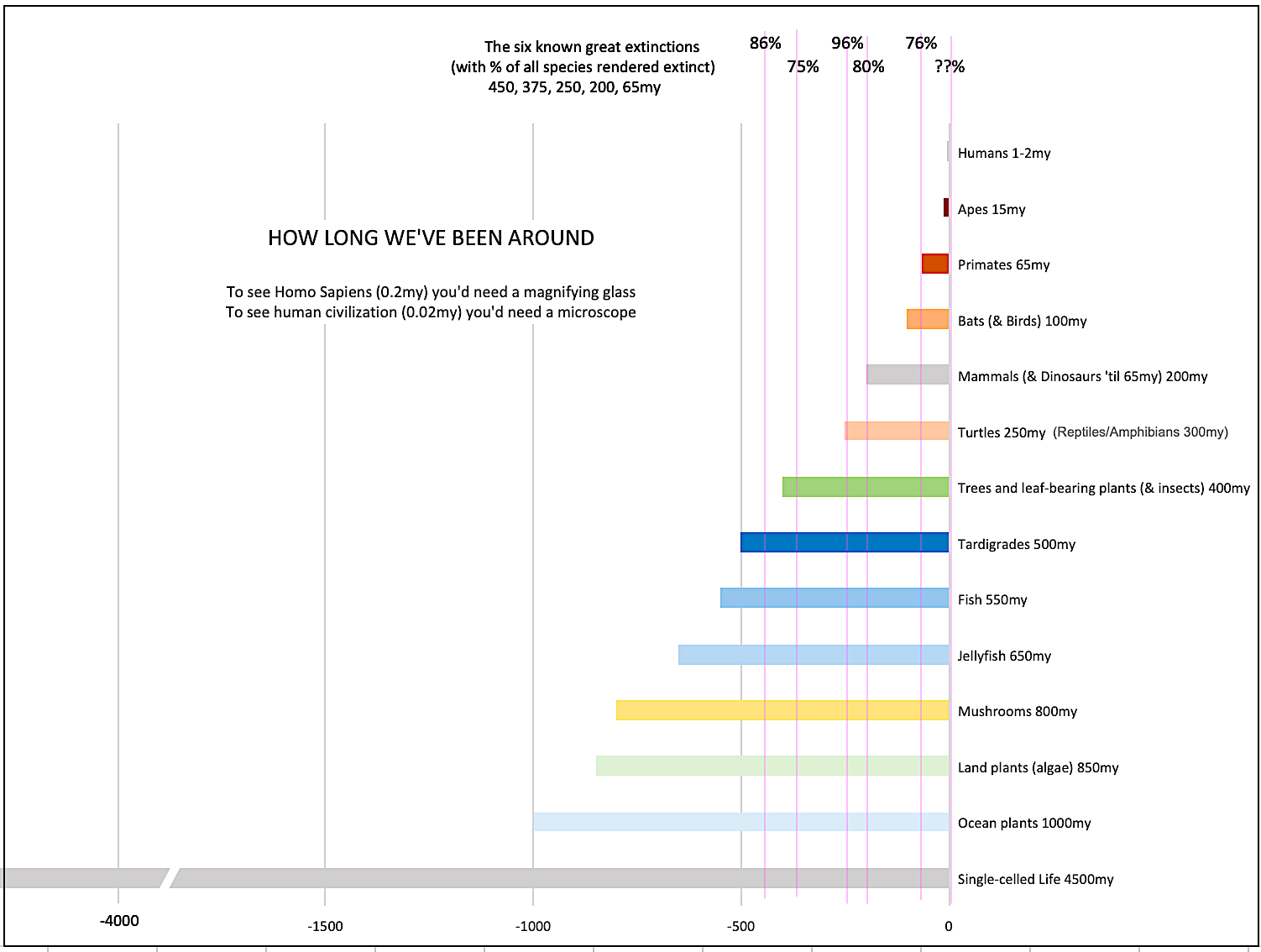
How Long We've Been Around (graphic)
If You Wanted to Sabotage the Elections
Collective Intelligence & Complexity
Ten Things I Wish I'd Learned Earlier
The Problem With Systems
Against Hope (Video)
The Admission of Necessary Ignorance
Several Short Sentences About Jellyfish
Loren Eiseley, in Verse
A Synopsis of 'Finding the Sweet Spot'
Learning from Indigenous Cultures
The Gift Economy
The Job of the Media
The Wal-Mart Dilemma
The Illusion of the Separate Self, and Free Will:
No Free Will, No Freedom
The Other Side of 'No Me'
This Body Takes Me For a Walk
The Only One Who Really Knew Me
No Free Will — Fightin' Words
The Paradox of the Self
A Radical Non-Duality FAQ
What We Think We Know
Bark Bark Bark Bark Bark Bark Bark
Healing From Ourselves
The Entanglement Hypothesis
Nothing Needs to Happen
Nothing to Say About This
What I Wanted to Believe
A Continuous Reassemblage of Meaning
No Choice But to Misbehave
What's Apparently Happening
A Different Kind of Animal
Happy Now?
This Creature
Did Early Humans Have Selves?
Nothing On Offer Here
Even Simpler and More Hopeless Than That
Glimpses
How Our Bodies Sense the World
Fragments
What Happens in Vagus
We Have No Choice
Never Comfortable in the Skin of Self
Letting Go of the Story of Me
All There Is, Is This
A Theory of No Mind
Creative Works:
Mindful Wanderings (Reflections) (Archive)
A Prayer to No One
Frogs' Hollow (Short Story)
We Do What We Do (Poem)
Negative Assertions (Poem)
Reminder (Short Story)
A Canadian Sorry (Satire)
Under No Illusions (Short Story)
The Ever-Stranger (Poem)
The Fortune Teller (Short Story)
Non-Duality Dude (Play)
Your Self: An Owner's Manual (Satire)
All the Things I Thought I Knew (Short Story)
On the Shoulders of Giants (Short Story)
Improv (Poem)
Calling the Cage Freedom (Short Story)
Rune (Poem)
Only This (Poem)
The Other Extinction (Short Story)
Invisible (Poem)
Disruption (Short Story)
A Thought-Less Experiment (Poem)
Speaking Grosbeak (Short Story)
The Only Way There (Short Story)
The Wild Man (Short Story)
Flywheel (Short Story)
The Opposite of Presence (Satire)
How to Make Love Last (Poem)
The Horses' Bodies (Poem)
Enough (Lament)
Distracted (Short Story)
Worse, Still (Poem)
Conjurer (Satire)
A Conversation (Short Story)
Farewell to Albion (Poem)
My Other Sites

{kind=link}
{kind=link}
Hi Dave, I love your blog, although this post is not one I would normally comment on, however I would like to know what you use to produce the great diagrams!
Mornig DaveThis is where we are going (Robin and I) I think that it is inevitable. More and more people I come into contact with tell me how their regimen of drugs has in the end made them more ill. But merely gossiping with each other is not as good as becoming truly informed. Hence your idea of the Exchange. I wonder how such an exchange could be started? What would be the essence of its core that would ensure that it could be trusted?
As a medical student, the current healthcare situation certainly concerns and distresses me greatly. I would love to see a peer-reviewed and moderated “Medipedia” much like Wikipedia on the internet, which I think would be as close to your idea of a non-profit, unbiased source of information. If I had any skills in the computer sciences (I am incredibly electronically inept), I would start one. While there are many databases out there, each has an agenda and so some patients are wary of them (and some sites deserve wariness), including the government-based sites. I tihnk the peer moderation would be more difficult than some Wikipedia entries (“governors of new jersey”), but less than many others (“evolution”), so I see it as a very feasible possibility.
I think a core element here is the ability to define and manage the information and interaction flow in relation to your own ongoing care. Key to this (in turn) is the trusted source, and the value you place on their insights, advice etc. Finally, the blind spot: their are ways in which we could “volunteer” our information to others so that we can be monitored (i.e. I am dieting, excercising and not loosing weight, my sisters are, what’s wrong? your designated coach sees the grocery list, your daily food log, and your excercise data from the gym, and hey, you know your not actually going to the gym as much as you think!). Simplistic example, but at its core is the ability to nominate other network participants to “med-i-digg” you, so that you have some soft of control over those blind spots.